Whole grain (Q&A)
Last Updated : 26 October 2023Eating whole grains as part of a healthy diet may help to reduce the risk of many common diseases. This article explores common questions about whole grains, shedding light on their nutritional value, types, and how they contribute to a healthy lifestyle. You will also find easy tips on how to identify whole grain products and increase your everyday consumption.
What is a whole grain?
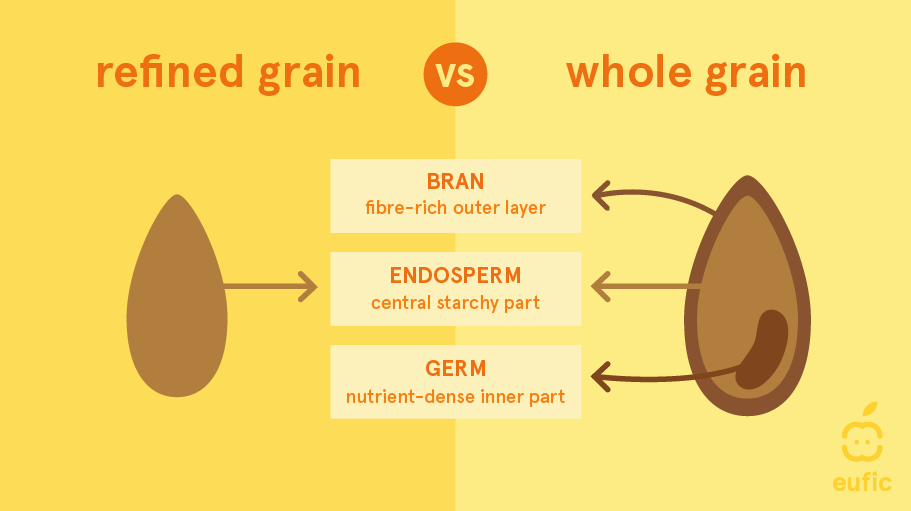
Whole grain refers to an entire cereal grain, also known as a kernel. The kernel consists of three elements:1
- the bran: a fibre-rich outer layer of a kernel (12-17%)
- the germ: a nutrient-dense inner part of a kernel (approximately 3%)
- the endosperm: a central starchy part of a kernel (80-85%)
To be defined as ‘whole grain’, a food product must retain the same relative proportions of its components (bran, germ, and endosperm) as they exist in the intact grain.
What is the difference between whole grains, refined grains, enriched grains and multigrain?
- Whole grains include the entire kernel (see above). They are either eaten whole, as a single food (such as wild rice or popcorn), or cracked, crushed, or flaked, as an ingredient in foods (such as in cereals, breads, and crackers). Some examples of whole grains include buckwheat, bulgur, millet, oatmeal, quinoa, rolled oats, brown or wild rice, wholegrain barley, whole rye, and whole wheat.
- Refined grains have been milled to remove the bran and germ from the grain. This results in grains having a finer texture and better shelf life. However, the milling also removes dietary fibre and other bioactive compounds that are mainly present in the bran and germ.
- Enriched grains are grain products with added B vitamins (thiamine, riboflavin, niacin, folic acid) and iron. The enrichment process involves adding nutrients that were originally present in the food but lost during food processing.
- Multigrain means that the product contains more than one type of grain, but it does not necessarily mean that the product is whole grain.2
What nutrients are present in whole grain?
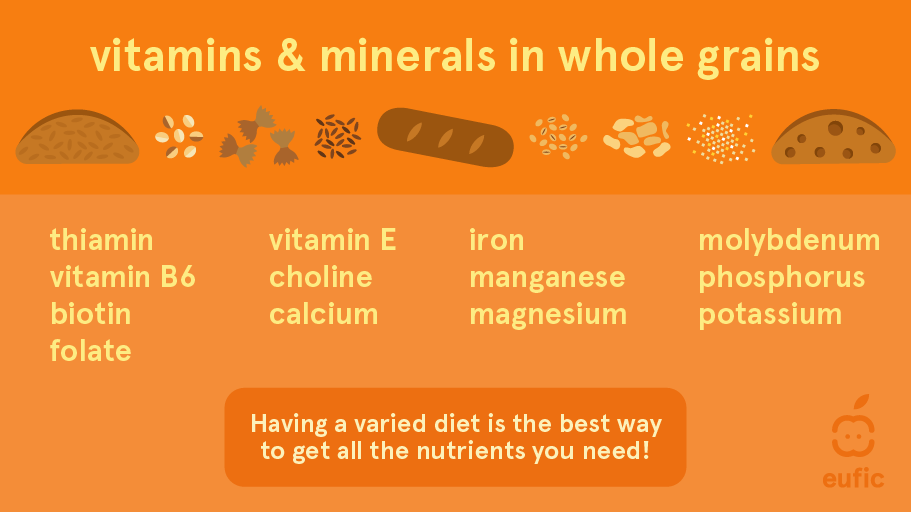
Whole grain is a rich source of bioactive nutrients including both soluble (for example β-Glucan) and insoluble (for example lignin) dietary fibre, B vitamins, trace minerals and phytochemicals.1 Whole grain foods can contain up to 75% more nutrients than refined cereals.3
The most beneficial part of grains is in the outer bran, followed by the germ of the seed.
- The bran contains fibre, minerals such as iron, zinc, copper and magnesium, vitamin E, B vitamins, and a multitude of other bioactive compounds (e.g., flavonoids, carotenoids).
- The germ contains essential unsaturated fats, B vitamins, vitamin E, selenium, antioxidants, plant sterols, and other bioactive compounds.
- Endosperm is a starchy part of a grain and contains largely carbohydrates, some proteins, and small amounts of fibre (e.g., β-Glucan), vitamins and minerals such as selenium, B vitamins, and vitamin E.1
What whole grains are high in fibre?
Whole grains have high levels of bran, giving them high amounts of fibre. In the table below you can find how much fibre several types of whole grain contain.4
|
|
Dietary fibre, per 100 g |
|
Whole grain barley (uncooked) |
14.8 |
|
Rye flour |
14.8 |
|
Bulgur (uncooked) |
12.5 |
|
Whole wheat flour |
10.3 |
|
Rye bread |
8.2 |
|
Oatmeal |
7.3 |
|
Quinoa (uncooked) |
7 |
|
Whole grain pasta (uncooked) |
6.9 |
|
Whole wheat bread |
6.7 |
|
Buckwheat |
5.6 |
|
Millet (uncooked) |
3 |
|
Brown rice (uncooked) |
3 |
Why is eating whole grain important?
There is growing evidence that eating whole grain products regularly as part of a healthy diet and lifestyle may help to reduce the risk of many common diseases. A high intake of whole grains lowers the risks of non-communicable diseases such as cardiovascular diseases, type 2 diabetes, and colorectal cancer. Whole grains also play a role in weight management.
A low intake of whole grains is the leading dietary risk factor for the number of years lost due to ill-health, disability, or early death in Europe. In 2019, a diet low whole grain was attributable to over 9.6 million disability-adjusted life years (or 3.17% of total disability-adjusted life years), a metric which represents the total burden of disease – both from years of life lost and years lived with a disability.5
Cardiovascular disease
Observational studies consistently show that eating whole grains reduces the risk of cardiovascular disease and stroke.6 Pooled results from available randomised controlled trials also show that a higher whole grain intake reduced serum cholesterol and low-density lipoprotein (LDL) cholesterol, two risk factors for cardiovascular disease in study participants. The phytochemicals in whole grains could also help in reducing blood pressure.7
Cancer
The World Cancer Research Fund states that there is strong evidence that whole grains decrease the risk of colorectal cancer.8 For every 90 g per day of whole grain consumption, the risk of colorectal cancer decreases by 17%. Whole grains may protect against colorectal cancer by binding carcinogens, regulating glycaemic response, and/or because of the anti-carcinogenic properties of the wide variety of nutrients they contain. For other types of cancers there were too few studies available to assess the relationship with certainty.
Type 2 diabetes
There is convincing evidence that higher whole grain intakes decrease the risk of type 2 diabetes. Results from four meta-analyses concluded that daily whole grain intakes of 2 or 3 servings (30-45 g per day) can significantly reduce the incidence of developing type 2 diabetes (20 to 32% lower risk).9 This may be due to the insoluble fibre content of whole grains which delays how fast foods moves from your stomach to your small intestine and decreases the time it takes for glucose to be absorbed in your cells. Both these factors have a positive effect on glucose and insulin responses.
Weight management
Whole grains seem to be beneficial in maintaining a healthy body weight over time as part of a healthy diet and lifestyle. Whole grains are usually low in fat, but rich in fibre and starchy carbohydrate. Some have also a low glycaemic index (GI), which means they provide a slow release of carbohydrate into the blood. This, together with fibre content, may help to keep you feeling fuller for longer - helping to control appetite.10 There is data to suggest that whole grain consumption can lead to slightly reduced body weight in obese/overweight populations compared to non-whole grain diets.11
What is a daily recommended whole grain intake?
The recommended daily intake of whole grains varies between countries. Most European food-based dietary guidelines recommend that refined cereals should be replaced by whole grains, with no recommendations on the exact recommend daily intake.12 Other European guidelines, such as the Nordic Nutrition Recommendations, recommend having an intake of at least 90 g (dry weight) per day of whole grains (preferably whole grain cereals other than rice).13
Why is whole grain better than white?
Whole grains are more nutritious compared to white, refined grains due to their intact grain kernel – bran, endosperm and germ which provide nutrients like fibre, vitamins, minerals, and antioxidants. This nutritional complexity offers several benefits over refined grains, where the bran and germ are removed during processing.
A 2020 meta-analysis concluded that replacing refined grains with whole grains can improve several risk factors for cardiovascular disease, including total cholesterol, low-density lipoprotein (LDL) cholesterol and haemoglobin A1c (a long-term marker of average blood sugar levels, used to measure diabetes control), although they mentioned that more interventional evidence is needed.14 Other reviews also show that refined grains do not have similar beneficial associations compared with whole grains.13
Can whole grain cause gas or constipation?
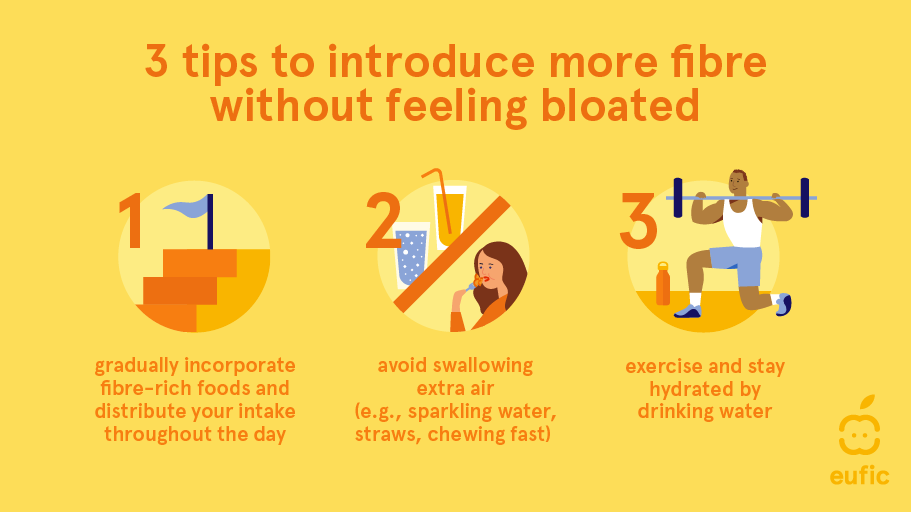
While whole grains are highly nutritious and beneficial for digestive health, the high fibre content can make them difficult to digest for some people. This can lead to gas or bloating, especially for people who are not used to a high-fibre diet. Fibre gets fermented in your digestive system which produced gasses and therefore can cause bloating (as a normal response). However, we can retrain our gut to embrace more fibre with a few simple tips:
- Gradually incorporate fibre-rich foods and distribute intake throughout the day
- Avoid swallowing extra air (e.g., chewing fast)
- Exercise and stay hydrated by drinking water
If you experience persistent or severe digestive issue, consult a healthcare professional (e.g., GP or registered dietitian/nutritionist) for personalised advice.
How to select the whole grain product?
To know whether a product contains whole grain, check the ingredients list on product labels for the words ‘whole’ or ‘wholegrain’ before the name of the cereal, for example ‘whole wheat pasta’ or ‘whole oats’. If whole grains are the first or second ingredient, after water, the food is generally considered whole grain.
Another practical rule when choosing whole grain products (e.g., breads, breakfast cereals, crackers, granola, cereal bars) is to look at the nutrition declaration: for every 10 g of carbohydrate there should be at least one gram of fibre. For example, if a bread has 45 g of carbohydrates per 100 g, it should contain at least 4.5 g of fibre. This 10:1 ratio is approximately equal to the carbohydrate to fibre content of whole wheat flour. Thus, it can broadly estimate if a product is whole grain, although it cannot distinguish between naturally occurring fibre from whole grains versus added fibre alone, which may have less health benefits compared with whole grains. Nevertheless, this ratio is a useful measure to identify healthful whole grain products as foods that met the 10:1 ratio also tended to have less sugar and sodium than those that didn’t. In the same study, products where whole grains were the first ingredient or where ‘whole’ was mentioned before the name of the cereal also tended to contain less sodium, but also more sugar and kcal.15
Foods labelled with the words ‘multi-grain’, ‘stone-ground’, ‘100% wheat’, ‘seven-grain’, or ‘bran’ are usually not 100% whole grain products and may not even contain any whole grains. Colour alone is also not a good indicator of a whole grain product. For example, bread can be brown because of molasses or other colouring ingredients.1
Is whole wheat whole grain?
Whole wheat is a whole grain. Whole wheat is derived from the entire wheat kernel, including the bran, germ, and endosperm. If a product retains all three parts of the wheat kernel (in the same relative proportions), they can be considered whole grains and as such are rich in fibre, vitamins, minerals, and other nutrients.
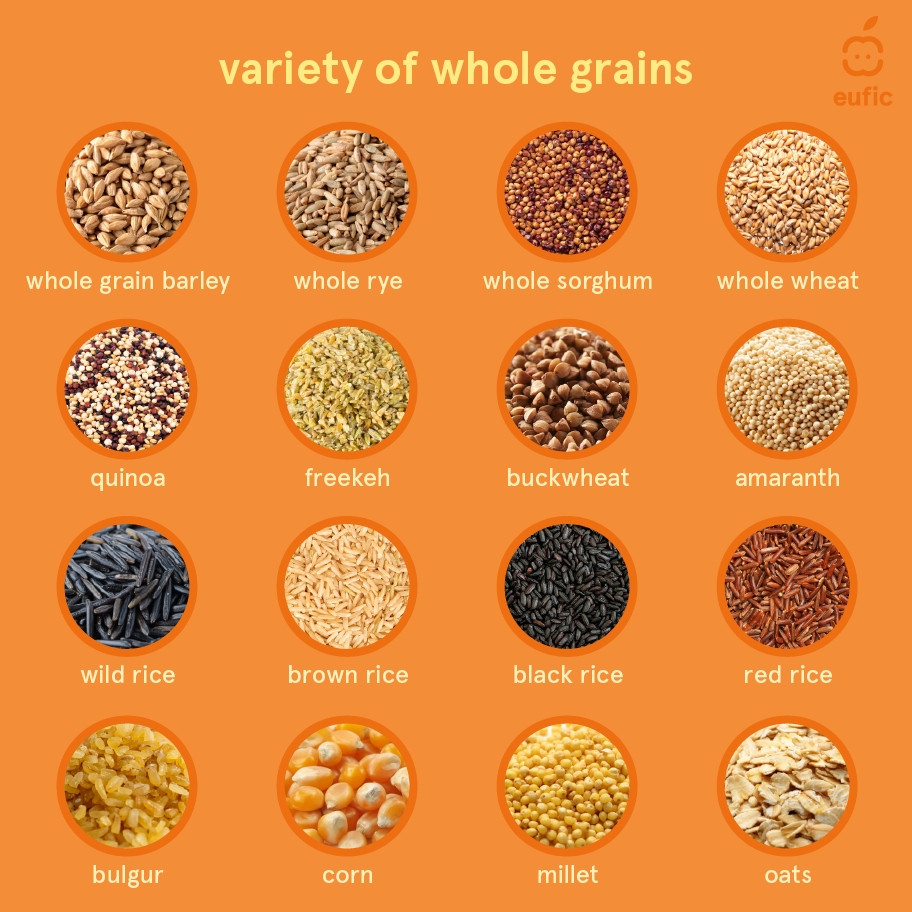
What are examples of whole grain products?
Examples of whole grains include whole grain barley, bulgur, corn, freekeh, millet, oats, brown, black, red, or wild rice, whole rye, whole sorghum, teff, and whole wheat (including wheat varieties like Einkorn, whole Farro/Emmer, and whole spelt). The pseudo-cereals (i.e., crops with a similar nutritional profile and uses to ‘true’ cereal grains) amaranth, buckwheat, and quinoa are also whole grain.16 There is not one whole grain that is best for health. All whole grains are good for health and provide different nutrients. The key to a healthy diet is diversity and including a mix of whole grains to reap the diverse benefits they offer.
Can whole grain be gluten-free?
Several whole grains are gluten-free. Gluten is the name given to the protein found in some, but not all grains:
- Grains containing gluten include: wheat, barley, bulgur, rye, and oats.
- Gluten-free (pseudo-)grains include: corn, millet, rice, sorghum, amaranth, buckwheat, quinoa, teff, and certified gluten-free oats.
If a gluten-containing grain is used in the production of a food, then the gluten source must be clearly stated on the label (e.g., in italic, underlined, or bold). However, remember, there is no evidence that gluten-free diets are beneficial for people for who don’t have a gluten-related disorder. Some gluten-free products may even have higher amounts of sugar, fat, or salt than the conventional versions and may not be healthier alternatives.
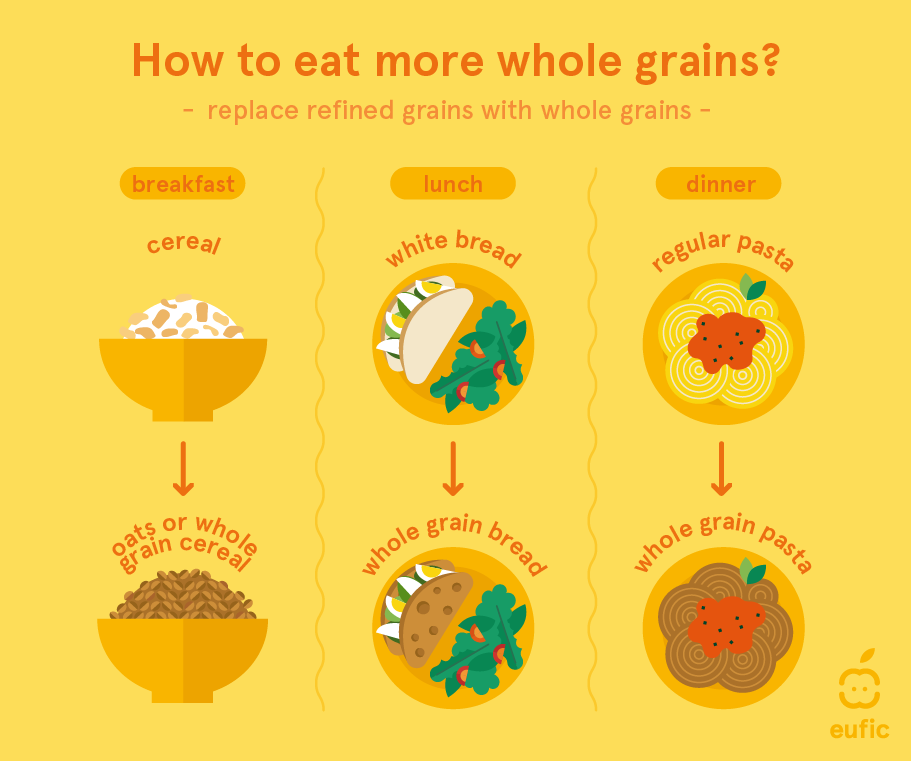
How can I eat more whole grains?
When choosing foods from the starchy food group, replace refined cereal foods, such as white bread, rice, and pasta, with whole grain varieties such as whole-meal bread, brown rice and wholewheat pasta. Wheat, oats, barley, rye, and rice are the most commonly available cereals which can be eaten in the whole grain form. It is important to replace the refined grain product for the whole one, rather than just adding the whole grain product to your existing diet.3
References
- Healthgrain Forum. (2023). Whole grain. Accessed 17 October 2023
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. (2010). Dietary Guidelines for Americans, 2010. 7th Edition, Washington, DC: U.S. Government Printing Office, December 2010
- The Association of UK dietitians. (2022). Wholegrains. Accessed 17 October 2023
- Dutch Food Composition Database (NEVO). NEVO-online version 2021/7.1. Accessed 04 October 2023
- IHME. (2019). Global Burden of Disease. Accessed 4 October 2023.
- McRae, M. P. (2017). Health benefits of dietary whole grains: an umbrella review of meta-analyses. Journal of chiropractic medicine, 16(1), 10-18.
- Biesinger S, Michaels HA, Quadros AS, et al. A combination of isolated phytochemicals and botanical extracts lowers diastolic blood pressure in a randomized controlled trial of hypertensive subjects. Clin Nutr. 2016;70(1):10-16.
- World Cancer Research Fund International. (2018). Wholegrains, vegetables and fruit and the risk of cancer. Continuous Update Project Expert Report.
- McRae, M. P. (2017). Health benefits of dietary whole grains: an umbrella review of meta-analyses. Journal of chiropractic medicine, 16(1), 10-18.
- Giacco R, Della Pepa G, Luongo D, et al.(2011). Whole grain intake in relation to body weight: from epidemiological evidence to clinical trials. Nutrition, Metabolism and Cardiovascular Diseases 21(12):901-8
- Wang, W., Li, J., Chen, X., Yu, M., Pan, Q., & Guo, L. (2020). Whole grain food diet slightly reduces cardiovascular risks in obese/overweight adults: a systematic review and meta-analysis. BMC cardiovascular disorders, 20, 1-11.
- European Commission. (2021). Dietary recommendations for whole grain intake. Accessed 4 October 2023
- Blomhoff, R., Andersen, R., Arnesen, E. K., Christensen, J. J., Eneroth, H., Erkkola, M., ... & Trolle, E. (2023). Nordic Nutrition Recommendations 2023: Integrating Environmental Aspects.
- Marshall, S., Petocz, P., Duve, E., Abbott, K., Cassettari, T., Blumfield, M., & Fayet-Moore, F. (2020). The effect of replacing refined grains with whole grains on cardiovascular risk factors: a systematic review and meta-analysis of randomized contro
- Mozaffarian, R. S., Lee, R. M., Kennedy, M. A., Ludwig, D. S., Mozaffarian, D., & Gortmaker, S. L. (2013). Identifying whole grain foods: a comparison of different approaches for selecting more healthful whole grain products. Public health nutrition, 1
- Whole Grains Council. (2023). Whole grains A to Z. Accessed 04 October 2023.